
Juvenile Nasopharyngeal Angiofibroma is a benign tumour consists of fibrous tissue with a variable proportion of vascular tissues occur in the nasopharynx of mainly prepubertal and adolescent male. At first Hippocrates described this tumour in the 5th century BC but Friedberg first used the term Angiofibroma in 1940. Other titles (eg, nasopharyngeal fibroma, bleeding fibroma of adolescence, fibroangioma) have also been used. It accounts for only 0.05% of all head and Neck tumor’s, but yet dangerous. It used to happen predominantly and exclusively in male of teen ages with age ranges between 7 to 19 years with a peak in 14 years rare in patients older than 25 years.
For Nonmedical Person, It is not wise to go through the Etiology and Pathology part, I think its quite hard.
Etiology:
The tumors arises from the posterolateral wall of the nasal cavity and superolateral nasopharyngeal wall with close proximity to the Sphenopalatine foramen which is considered as the specific site of the origin of the tumour. Hormonal theory (testosterone) is suggested for this disease as it occurs predominantly in Male child. Other theories includes a Desmoplastic response of the nasopharyngeal periosteum or the embryonic fibro cartilage between the basioocciput and the basisphenoid.
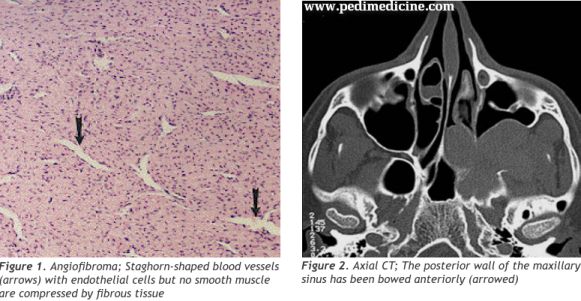
Pathology:
As the tumour expands it erodes the surrounding structure. It may expands laterally into the pterygopalatine fossa through the pterygomaxillary fissure and into the infratemporal fossa. Or may expands superiorly to erode the pterygoid plates, the greater wings of sphenoid and the skull base foramina. Anterosuperior expansion into the nasal cavity, paranasal sinuses and orbit may also occur.
Symptoms:
- Nasal Obstruction
- Epistaxis that means bleeding from the nose mostly unilateral and recurrent.
- Facial Swelling.
- Broadening of the nasal bridge, unilateral cheek prominence and displacement of the Globe of the eye commonly known as Frog face Deformity.
- Headache
- Nasal discharge.
- Other’s include deafness and cheek swelling.
Signs:
- Smooth firm reddish or pinkish polypoid unilateral nasal or nasopharyngeal mass.
- Proptosis which means forward displacement of eye (Also found in Graves disease).
- Otitis media with effusion.
Investigations:
Diagnosis is mainly done from clicnical features and the observation of a Otolaryngologist Surgeon. Further investigations may help to confirm the diagnosis and establish the cause and origin.
- X-ray Nasopharynx Lateral view And Paranasal Sinus Occipitomental view give a idea about the extension of disease.
- An MRI with STIR sequence is the investigation of choice to define the extent and vascularity of the tumour.
- Large vascular tumour needs Digital subtraction angiography for identifying and embolizing feeding vessels.
Treatment:
Todays patients and the relatives are curious about the disease. It also necessary to raise the concern about the prognosis and follow up. All treatment options including Medical therapy, Surgical or Chemo radiation needs their understanding. So a surgeon must tell them as necessary.
Medical Therapy:
- External Beam radiotherapy (30-40Gy) is for unresectable, intracranial or recurrent diseases.
- Chemotherapy: A non steroidal androgen blocker, Flutamide that interferes with the testosterone binding has been found effective to reduce tumour size.
- Hormonal therapy with Diethylstilbestrol (5mg TDS for 6 Weeks) 2-3 weeks before surgery has been shown to reduce the vascularity before excision.
Surgical Treatment:
Surgical therapy is the treatment of choice. Medical therapy is used to reduce the size and vascularity before excision. Different surgical approaces are available depending on the tumour size and extension. Combination of approaches may be used depending on the choice of surgeon.
Transpalatal (Small tumour in nasopharynx)
Midfacial degloving.
Lateral Rhinotomy and lipsplitting
Transantral or transzygomatic infratemporal approach
Craniofacial resection if cribiriform plate is involved.
Weber-Ferguson incision is done for removal of lesions at the entry of the nasal passage.
Complications are related with intracranial extension or extensive bleeding
Follow up:
You need to keep contact with your surgeon in case of recurrence. Development of bleeding from the nose or nasal obstruction may raise the suspicion. Recurrence are treaded with radiotherapy or reoperation.
Ok that’s for today. Thanks.
I am an Iranian and I live in Tehran and 26 years old, 10 years that I have stains on my face i have to ask you what type of therapy will eliminate the stains on the face of the replies to the e-mail I send grateful thanks