
Congenital Birth Defects are quite common. When a congenital birth defect is found Physicians have to make sure there are no other defects. Congenital birth defects or congenital anomalies are of various types. Some of them require urgent medical attention and some of them, surgical intervention. Few congenital birth defects do not require any treatment at birth. A few days ago an inborn baby admitted in our NICU with multiple congenital birth defects. This is a case history of a baby with multiple congenital birth defects.

Son of M, 1900 gram birth weight admitted to our NICU just after birth due to respiratory distress and multiple congenital anomalies. The baby was born by LUCS at 36th weeks of gestation due to premature rupture of membrane for 8 hours. The baby cried immediately after birth but developed respiratory distress and cyanosis.
Mother Mrs. M, 36 years old elderly primigravidae blood group AB positive having a history of IVF and subfertility. She was taking Tab. Thyroxin for hypothyroidism. She was under regular antenatal checkup and her pregnancy period was uneventful till now.
On Admission the baby was ill-looking, dyspneic, cyanosed and having poor reflex activity. Regarding vital signs, Heart rate 136 /min, respiratory rate 48/min, temp normal with the cold periphery. Air entry on both lung field was moderate. Heart sound was found normal. Fontanelle was open and at the level. Umbilicus was healthy.
The baby had following congenital birth defects


- Extra digit on the right thumb.
- Undescended testis but that’s normal unless other defects present.
- Imperforated anus.
- Meconium passing from the urethra indicating rectourinary fistula.
- Sacral pit.
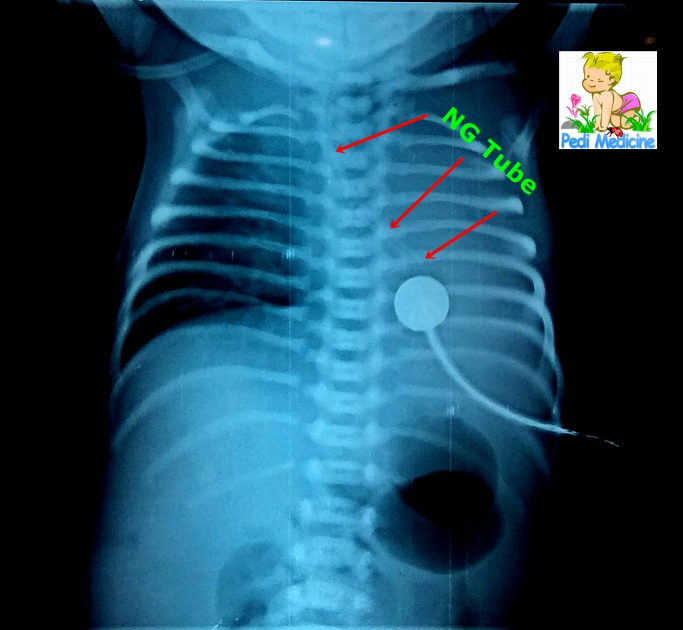
- NG tube was not passing through esophagus and there was profuse secretion, so esophageal atresia or tracheoesophageal fistula was suspected.
- The congenital diaphragmatic hernia was suspected due to respiratory distress.
Other system examination revealed no apparent congenital malformations.
Provisional Diagnosis:
Pre-Term (36th weeks) with LBW (1900gm) with Multiple Congenital Anomalies.
Investigation Reports:
Contrast Shallow Esophagus: Upper third of the esophagus was outlined by the contrast with the moderately dilated blind end. No contrast is visualized in the rest of the esophagus and stomach. Evidence of contrast is seen in the trachea and bronchial tree through a fistulous communication with the proximal part of the esophagus and trachea.

Echocardiography Report:
- Moderate perimembranous VSD
- Closing PDA
- Persistent Foramen Ovale
- Dilated LA and LV
- Moderate PAH
- TR Grade 1
Babygram: The rectum as a whole is devoid of any air up to anal verge. There is no evidence of any spina bifida or meningocele.

Ultrasonogram report:
Spine: the spine appears normal, however, the coccyx is not well seen in USG. The area of anal pit corresponds to the extension of lower end of spinal canal fluid, just beneath the skin.
Anal canal: the blind pouch of the anal canal is 10.6 mm at depth of from the perineum, which is borderline between a high and low variety of anorectal malformation.
Abdomen: The ascending colon. sigmoid colon and rectum are mildly distended and shows the presence of echogenic debris. The distance of the lower end of the anal canal to the perineum is about 1.02 cm. Other findings are normal.
Other hematological investigation reports were insignificant.

Treatment:
The baby has managed accordingly with Oxygen inhalation, IV fluid, broad-spectrum antibiotics, and other supportive measurements. The pediatric surgeon visited the baby later and advised on thorough investigations and suggested surgical intervention. Right transverse colostomy was done at 3rd days of age and the baby was put under mechanical ventilation for 2 days. Contrast Xray esophagogram revealed esophageal atresia with tracheoesophageal fistula. The spinal cord was intact. There was no congenital diaphragmatic hernia. The baby was shifted to a Govt Hospital for further treatment upon request of the concerned parent’s party.
See Also: SMA Birth Defect (Spinal Muscular Atrophy)
Resources of Congenital Birth Defects:
Birth Defects Are Preventable by www.ncbi.nlm.nih.gov
Birth defect Wikipedia
About one in every 33 babies is born with a birth defect. Not all birth defects can be prevented. But a woman can take steps to increase her chance of having a baby with the best health possible. Birth Defects by CDC
Download this page as PDF
Thanks.
